
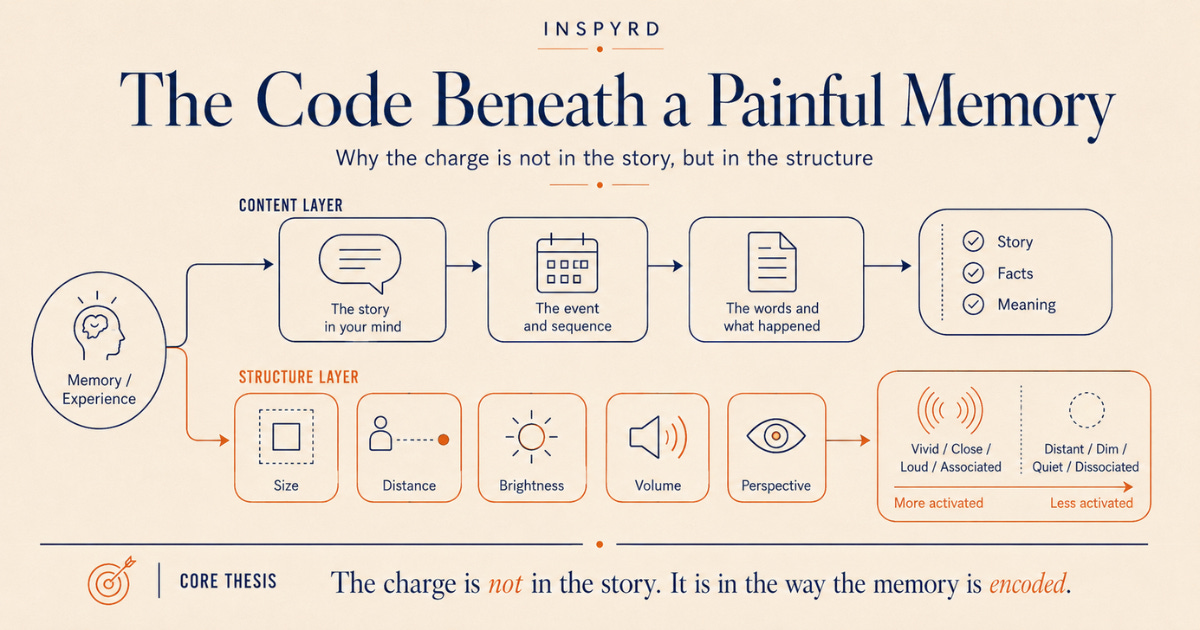
The Code Beneath a Painful Memory
Why the charge is not in the story itself, but in the sensory structure the nervous system is still running.

This article is adapted from the INSPYRD library as part of the Affective Memory Resolution series.
One of the things we get wrong about a painful memory is that we focus on what it is about.
The content is not what is running.
The structure is.
The size of it. The distance. The brightness. The volume. The code beneath the content.
This is Pillar 6 of the INSPYRD framework. In the previous article, I argued that REM sleep is the nervous system’s overnight integrator of emotional memory, replaying emotional content with noradrenaline suppressed and depotentiating the affective charge while the memory is offline. That account raised a structural question. If the integration is a replay, what is the format of the replay? What is the actual code the brain uses to hold an experience. And to change it?
The answer is the most precise lever available in waking change work. And it sits beneath the content as the layer that actually carries the charge.
Charge is not in the content.
It is not in the meaning.
It is not in the words.
It is in the structure.
If we are going to repair an injury, we have to be precise about the layer the injury is encoded in.
A memory has two layers
Every internal experience has two layers, and conflating them is the most common reason change work stalls.
There is the content. What the memory is of. The event, the people, the words, the sequence. And there is the structure. How the memory is coded. Most clinical and coaching approaches work almost entirely on the content. They ask what happened, what it meant, what the client now believes about it. That work is not worthless. But the content is not what carries the charge.
The structure is.
What submodalities are
The brain codes every internal representation in sensory parameters. A remembered image has a size, a location in the visual field, a distance from the observer, a brightness, a degree of colour saturation, a quality of motion or stillness. A remembered sound has a volume, a spatial location, a tone, a tempo. A felt sensation has a place in the body, a temperature, a weight, a direction of movement.
These structural parameters are called submodalities. They sit beneath the content as the code the nervous system actually runs.
The clinical fact that makes this matter: the charge of a memory is carried by its submodalities, not by its content. Take a single memory and run it as a large, bright, close, moving image with loud associated sound. Then run the same memory, same event, same content, as a small, dim, distant, still image with the sound turned down. The content has not changed. The charge has. The nervous system is not responding to what happened. It is responding to how what happened is currently coded.
Drivers: why this is precise, not general
Not every submodality carries equal weight. For any given memory in any given person, one or two submodalities carry most of the charge. These are the drivers. For one client the driver is distance. For another it is brightness. For another it is the spatial location of a remembered voice. Identify the driver, shift the driver, and the whole representation reorganises around the change.
This is what makes submodality work a precision instrument rather than a blunt one. You are not trying to change everything about how a memory is held. You are finding the single structural parameter the charge is hanging on, and changing that.
The neuroscience underneath the construct
The idea that internal representations have a manipulable sensory structure is not folk psychology. It maps onto a well-established research base in cognitive neuroscience.
Stephen Kosslyn’s work established that mental imagery recruits the same neural substrate as perception. That picturing something and seeing something engage overlapping visual machinery. Nadine Dijkstra and colleagues took this further and showed that the vividness of a visual image depends specifically on the degree of neural overlap with perception in visual cortex. In other words, “vividness”, a submodality, has a measurable neural correlate. When a client reports a memory as intensely vivid, that report corresponds to a real, physical pattern of activation.
Emily Holmes and Andrew Mathews demonstrated that mental imagery has a privileged, amplified relationship with emotion compared to verbal representation of the same content. That imagining an event drives a stronger affective response than describing it. Ji, Heyes, MacLeod, and Holmes extended this into the model of emotional mental imagery as a simulation of reality: the nervous system treats a sufficiently structured internal representation as though it were an external event. That is precisely why submodality structure has the leverage it has. The structure is what tells the nervous system whether it is dealing with a memory or with a present reality.
Why this connects to everything before it
Hold the through-line of the framework.
In Pillar 4, I argued that a traumatic memory is encoded without a time stamp. That the system runs it as present rather than past. Submodalities are that time stamp. A memory coded as close, vivid, large, and moving is coded as now. A memory coded as distant, faded, small, and still is coded as then. The structure is the temporal marker.
Memory reconsolidation is the biological window during which an activated memory becomes temporarily unstable and open to modification. When that window is open, part of what changes is the submodality structure. The code is what gets rewritten. And Visual-Spatial Tasking works, in part, because loading visual-spatial working memory degrades the visual submodalities of the activated memory while the window is open. Submodalities are not a separate technique sitting alongside Affective Memory Resolution. They are the encoding layer that AMR and VST operate on.
Association and dissociation
One submodality distinction is worth naming on its own, because it changes the entire physiological response to a memory with a single structural move.
Association is experiencing a memory through your own eyes, from inside it. Dissociation is seeing yourself in the memory, from the outside. Associated, the body runs the pattern. The autonomic response engages as though the event were present. Dissociated, the body has structural distance from it. This is not avoidance, and it is not suppression. It is a controlled change in the encoding structure, used deliberately, under regulation, as a defined step in the work.
What this means for practitioners
If you work with clients, the practical implications are direct.
When a client describes a memory, listen for structure, not just content. “It is right in my face.” “It is huge.” “I cannot get away from it.” “His voice is right here.” These are not figures of speech. They are submodality reports. The client is telling you, precisely, how the memory is coded. And therefore where the charge is.
Elicit before you intervene. Find the drivers before you change anything. A practitioner who changes submodalities at random is working blind; a practitioner who has identified the one or two drivers is working with precision.
And recognise which layer your training has equipped you to work on. If your training teaches you to work the content, the story, the meaning, the belief, you are working one layer up from where the charge lives. The clinical application of NLP, grounded in contemporary imagery neuroscience, is mechanism-first work at the structural layer. That is the layer where the change is precise, and where it holds.
Where this sits in the series
This is Pillar 6 of the INSPYRD framework. Pillar 4 established trauma as an encoding failure. Pillar 5 covered the overnight system that integrates emotional memory. Pillar 6 names the actual code that encoding is written in. Pillar 7, which comes next, examines language and cognitive framing. Because if submodalities are the sensory code, language is what directs the code. The words a client uses, and the words a practitioner uses, shape the structure directly.
One question before you go.
Of these three, which one matters most for someone you are working with right now?
Why is the memory so vivid, even years later?
Can you change a memory without losing it?
Or why do some memories fade and others do not?
Comment below. The next article in this series is built on what you tell me.
If you work with clients, this is the level we teach inside the INSPYRD certification.
If you want a lighter introduction, the AMR app walks you through the work experientially, and one-on-one work is available too.
FAQ
Why is the memory so vivid, even years later?
Because vividness is not a property of how recently something happened. It is a property of how the memory is structurally coded. A vivid memory is one with high-intensity submodalities: close, bright, large, loud. Years pass and the calendar moves, but the code can stay exactly the way it was the night it was laid down.
That is what people are pointing at when they say a memory “feels like yesterday”. The structure has not been updated. Time has moved. The code has not.
Can you change a memory without losing it?
Yes, and this is one of the most important distinctions in mechanism-first change work. You are not erasing the event. The content stays. What changes is the structure the content is held in. The memory remains accessible and accurate; the charge it was running gets updated.
Affective Memory Resolution works at that structural layer. The story can be remembered; the body no longer fires as though the event is current.
Why do some memories fade and others do not?
Most ordinary memories are integrated overnight in REM and gradually shift their structural code: more distant, dimmer, smaller, more still. That structural shift is what “fading” actually is. When the integration mechanism cannot run - for trauma-impacted nervous systems, it often cannot - the structural code stays at high intensity indefinitely.
The memory does not fade because the structure never moved.
What is a submodality driver, and why does it matter clinically?
A driver is the single submodality that carries most of the charge of a particular memory. For one client it might be distance, for another brightness, for another the spatial location of a remembered voice. Identifying the driver before intervening is the difference between working with precision and working blind.
Shift the driver and the whole representation reorganises around the change. Shift the wrong parameter and you waste a reconsolidation window.
Is this NLP or is it neuroscience?
Both, and the relationship is one-way. NLP supplied the original clinical construct of submodalities through Bandler’s practitioner work. Contemporary cognitive neuroscience, especially imagery research by Kosslyn, Dijkstra, Holmes, and Pearson, supplies the mechanistic grounding for why that clinical construct works.
The clinical application of NLP described here is NLP grounded in mainstream imagery neuroscience.
What is association and dissociation, in practical terms?
Association is experiencing a memory through your own eyes, from inside it. Dissociated is seeing yourself in the memory from the outside. Associated, the body runs the pattern as though the event is present. Dissociated, the body has structural distance from it.
Used deliberately and under regulation, the move from associated to dissociated is a controlled structural change. It is not avoidance.
Why is it not enough to talk about a memory in therapy?
Talking changes the content layer. The story, the meaning, the belief. The charge lives one layer down, in the structure. Talking about a memory can produce insight without changing its submodality code, which is why insight so often arrives without relief.
Mechanism-first work reaches the structural layer where the charge actually sits.
About the Author
Allen Kanerva is a trauma intervention trainer and the founder of INSPYRD. A former Royal Canadian Air Force tactical helicopter pilot, UN peacekeeping course director, and co-author of Canadian humanitarian security policy work, he developed Affective Memory Resolution (AMR) and Visual-Spatial Tasking (VST). A clinical protocol for nervous-system-level trauma resolution grounded in Hebbian learning and memory reconsolidation research. He trains practitioners internationally in NLP, trauma intervention, and mechanism-first change work.
ORCID iD: 0009-0009-1297-3778
Follow Allen on Substack and LinkedIn. Read more of the framework at blog.inspyrd.com.
References
1. Bandler (1985)
Bandler, R. (1985). Using your brain. For a change. Real People Press.
Annotation. The originating text for the submodalities construct in the NLP literature. Establishes the practical distinction between the content of an internal representation and its structural parameters, and the clinical observation that altering structure alters response. Cited as the primary-source origin of the construct this article grounds in contemporary neuroscience.
2. Dijkstra, Bosch, & van Gerven (2017)
Dijkstra, N., Bosch, S. E., & van Gerven, M. A. J. (2017). Vividness of visual imagery depends on the neural overlap with perception in visual areas. Journal of Neuroscience, 37(5), 1367-1373. https://doi.org/10.1523/JNEUROSCI.3022-16.2016
Annotation. Demonstrates that the vividness of a mental image, a submodality, corresponds to the degree of neural overlap between imagery and perception in visual cortex. Provides the direct neural correlate for the article’s claim that submodality intensity is a physical, measurable property of the representation, not a metaphor.
3. Holmes & Mathews (2010)
Holmes, E. A., & Mathews, A. (2010). Mental imagery in emotion and emotional disorders. Clinical Psychology Review, 30(3), 349-362. https://doi.org/10.1016/j.cpr.2010.01.001
Annotation. Reviews the evidence that mental imagery has a privileged, amplified relationship with emotion compared to verbal representation of the same content. Supports the article’s central claim that the structural-imagery layer, not the verbal-content layer, is where affective charge is carried.
4. Ji, Heyes, MacLeod, & Holmes (2016)
Ji, J. L., Heyes, S. B., MacLeod, C., & Holmes, E. A. (2016). Emotional mental imagery as simulation of reality: Fear and beyond. Behavior Therapy, 47(5), 702-719. https://doi.org/10.1016/j.beth.2015.11.004
Annotation. Articulates the model of emotional mental imagery as a simulation of reality. The nervous system treats a sufficiently structured internal representation as though it were an external event. Supplies the mechanistic reason submodality structure has the leverage it has: structure is what signals memory-versus-present-reality to the system.
5. Kosslyn, Ganis, & Thompson (2001)
Kosslyn, S. M., Ganis, G., & Thompson, W. L. (2001). Neural foundations of imagery. Nature Reviews Neuroscience, 2(9), 635-642. https://doi.org/10.1038/35090055
Annotation. Establishes that mental imagery recruits the same neural substrate as perception. Underwrites the article’s foundational premise that internal representations are processed by perceptual machinery, which is why their sensory structure is consequential and manipulable.
6. Pearson, Naselaris, Holmes, & Kosslyn (2015)
Pearson, J., Naselaris, T., Holmes, E. A., & Kosslyn, S. M. (2015). Mental imagery: Functional mechanisms and clinical applications. Trends in Cognitive Sciences, 19(10), 590-602. https://doi.org/10.1016/j.tics.2015.08.003
Annotation. Synthesises the functional mechanisms of mental imagery and connects them explicitly to clinical application. Supports the article’s bridge from the neuroscience of imagery structure to its use as a precision lever in mechanism-first change work.
I am a pharmacist but also severe abuse survivor. 7 years with tms and therapy have helped but certain memories still stick. ❤️🌈🙏💔